Information includes:
- Name and class of medication
- Indications for use
- Mechanism of action
- Side effects and interactions
- Route of administration
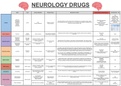
NEUROLOGY DRUGS
Name Class Clinical Indications Receptor Action Mechanism of Action Adverse Effects and Interactions Administration + PK
Oral
Bioavailability:
Morphine - 30%
Diamorphine - 30%
Codeine - 60%
Morphine Methadone - 80%
Respiratory depression
Diamorphine Morphine binding to opioid receptors blocks transmission of nociceptive signals, signals Due to heavy first pass
Addiction
Fentanyl
Opioids Remifentanil Opioid
Pain Selective μ-opioid pain-modulating neurons in the spinal cord, and inhibits primary afferent nociceptors to the Nausea and vomiting metabolism
Cough suppression receptor agonist dorsal horn sensory projection cells. Pupil constriction
Codeine
Histamine release (avoid in severe
Pethidine
asthmatics)
Methadone
Antagonises opioid receptors inhibiting the effect of opiate overdose such as respiratory Body aches
Opioid Non-selective competitive
Opioid antagonist Naloxone Opioid overdose depression Fever Nasal
antagonist opioid receptor antagonist
GI upset
Pramipexole
Non-ergot
Ropinirole Parkinson’s disease - added GI upset Initial dose of 88
dopamine
Rotigotine to levodopa if not sufficient to Orthostatic hypotension micrograms T.D.S
agonist
Apomorphine control symptoms D2 and D3 receptor Agonises D2 and D3 receptors in the striatum of the basal ganglia. This restores normal
Dopamine agonist motor function by acting as the dopamine that should be produced by the substantia nigra.
agonist Dose can be doubled
Bromocriptine Pramipexole for Restless Leg Fibrosis of heart, lungs and abdomen every week if tolerated
Ergot dopamine Syndrome up to 3.3mg/day max
Cabergoline Regular monitoring for cardiac fibrosis
agonist
Pergolide is needed throughout treatment
Levodopa crosses the blood brain barrier as the prodrug where it is then metabolised by
dopamine decarboxylase into dopamine. As dopamine, it binds to receptors in the direct and
indirect movement pathways of the basal ganglia, taking over the role of the dopamine that Drowsiness
Oral
Dopamine Non-selective dopamine should be produced by the substantia nigra, thereby restoring normal motor function. Seizures
Dopamine prodrug Levodopa Parkinson’s disease Typical starting dose of
prodrug receptor agonist Neuroleptic malignant syndrome
50mg T.D.S
Given alongside either carbidopa (co-careldopa) or benserazide (co-beneldopa) which Pathological gambling
inhibit peripheral dopamine decarboxylase only. This allows levodopa to reach the brain
without being metabolised first therefore lower doses can be given.
Rarely used due to many drug-drug
Inhibits MAO-B which is responsible for the breakdown of dopamine. By inhibiting the reactions
Parkinson’s disease - added
Rasagiline Monoamine oxidase B breakdown of dopamine, higher levels of dopamine are maintained, restoring normal motor Arrhythmias
MAO-B inhibitor MAO-B inhibitor to levodopa if not sufficient to Oral
Selegiline inhibitor function by acting on the direct and indirect movement pathways of the basal ganglia. Confusion
control symptoms
Orthostatic hypotension
Tyramine cheese reaction
GI upset
Parkinson’s disease - added
Entacapone Catechol-O-methyltransfe Inhibition of catechol-O-methyltransfe-rase prevents the peripheral breakdown of levodopa, Confusion
COMT inhibitor COMT inhibitor to levodopa if not sufficient to Oral
Tolcapone -rase inhibitor therefore enabling more levodopa to reach the brain. Fatigue
control symptoms
Red-brown urine
Advanced parkinson’s disease Not fully understood by increases pre-synaptic dopamine release and blocks dopamine
Corneal oedema Daily oral dose ranges
Amantadines Amantadine Amantadine when other treatments have Unknown reuptake.
Livedo reticularis from 100-400mg
failed
Diplopia, nystagmus, ataxia
Focal seizures
Inhibits voltage gated sodium channels, reducing neuronal depolarisation and therefore Hyponatraemia
Carbamazepine Generalised GTC seizure Voltage gated Na+ Oral
treating seizure activity. Rash
Oxcarbazepine Trigeminal neuralgia channel inhibitor 100-200mg b.d
May exacerbate absence, myoclonic
Bipolar disorder
Anticonvulsants Anticonvulsant and atonic seizures
T-type Ca2+ channel Inhibits semialdehyde dehydrogenase increasing GABAergic neurotransmission providing Avoid in women of child bearing age
Oral
Sodium valproate Men with any form of epilepsy inhibitor an inhibitory effect. Inhibits sodium and calcium channels, reducing neuronal depolarisation GI upset
300mg b.d
Na+ channel inhibitor and therefore treating seizure activity. Tremor
The benefits of buying summaries with Stuvia:
Guaranteed quality through customer reviews
Stuvia customers have reviewed more than 700,000 summaries. This how you know that you are buying the best documents.
Quick and easy check-out
You can quickly pay through credit card for the summaries. There is no membership needed.
Focus on what matters
Your fellow students write the study notes themselves, which is why the documents are always reliable and up-to-date. This ensures you quickly get to the core!
Frequently asked questions
What do I get when I buy this document?
You get a PDF, available immediately after your purchase. The purchased document is accessible anytime, anywhere and indefinitely through your profile.
Satisfaction guarantee: how does it work?
Our satisfaction guarantee ensures that you always find a study document that suits you well. You fill out a form, and our customer service team takes care of the rest.
Who am I buying these notes from?
Stuvia is a marketplace, so you are not buying this document from us, but from seller joey6. Stuvia facilitates payment to the seller.
Will I be stuck with a subscription?
No, you only buy these notes for £3.49. You're not tied to anything after your purchase.